The Paranoid Mind: Unmasking the Neuropsychiatric Epidemic of Cannabis-Induced Psychosis
The modern landscape of high-potency cannabis products poses a greater public health threat than the lower-potency products studied in previous decades.

Abstract
The escalating global trend toward cannabis legalization has brought into sharp focus the significant psychiatric adverse effects associated with its use, particularly cannabis-induced paranoia. This meta-research story synthesizes current evidence from epidemiological, neurobiological, and clinical studies to provide a comprehensive analysis of this phenomenon. Paranoia, existing on a spectrum from mild suspiciousness to severe persecutory ideation, represents one of the most distressing acute psychological effects of delta-9-tetrahydrocannabinol (THC), the primary psychoactive constituent of cannabis. The etiology is multifactorial, involving a complex interplay of dopaminergic and glutamatergic dysregulation, genetic vulnerabilities, pre-existing psychological conditions, and specific cannabis use patterns, notably high-potency THC product use. This story delineates the mechanisms underlying this condition, identifies critical risk factors, discusses clinical assessment strategies, and outlines imperative public health considerations aimed at mitigating this growing concern.
Introduction
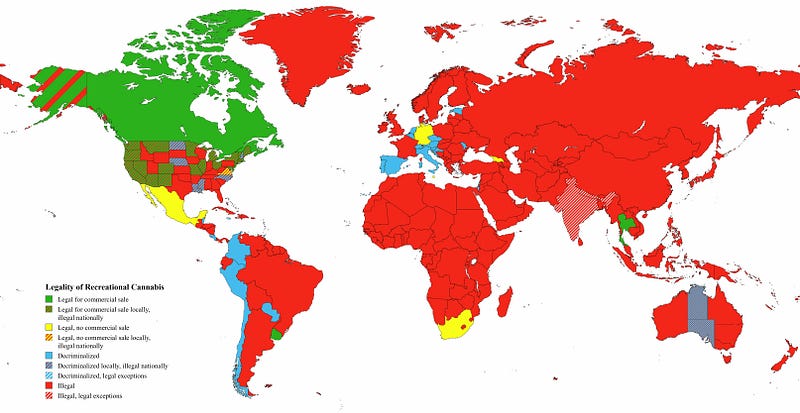
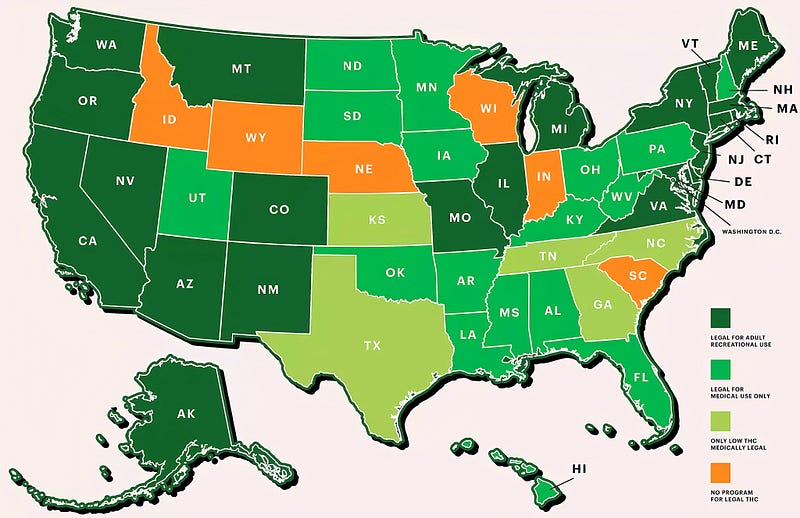
Cannabis remains the most widely consumed illicit substance globally, with its use becoming increasingly normalized through medicinal and recreational legalization efforts. Concurrently, clinical and epidemiological data reveal a substantial association between cannabis consumption and transient psychotic symptoms, with paranoia being the most commonly reported. The clinical significance of cannabis-induced paranoia extends beyond the acute intoxication period; evidence suggests that experiences of acute cannabis-induced psychosis may elevate the risk for the subsequent development of primary psychotic disorders. This story aims to consolidate the existing scientific literature to elucidate the prevalence, neuropsychological mechanisms, and moderating variables that govern the expression of paranoid ideation following cannabis exposure, providing a foundation for evidence-based clinical intervention and public health policy.
Neurobiological Mechanisms
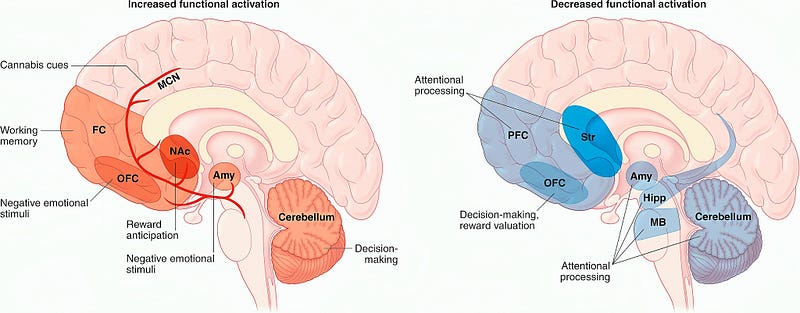
The psychotogenic properties of cannabis are predominantly attributed to THC, which acts as a partial agonist at cannabinoid CB1 receptors. These receptors are densely distributed throughout brain regions critical for emotional regulation, threat detection, and reality testing, including the prefrontal cortex, anterior cingulate, amygdala, and hippocampus. THC administration induces a dose-dependent dysregulation of dopaminergic signaling, particularly in the mesolimbic pathway, resulting in a hyperdopaminergic state that mirrors findings in primary psychotic disorders. This aberrant dopamine release is a hypothesized core mechanism for the formation of paranoid thoughts.
A study titled “How Cannabis Causes Paranoia” investigates the link between cannabis use and paranoia. The research involved the intravenous administration of 9-Tetrahydrocannabinol (THC), the primary psychoactive ingredient in cannabis, to 121 individuals with paranoid ideation. The results suggest that THC consumption increases paranoid ideation, and cognitive interventions can help mitigate these effects. The study sheds light on the cognitive mechanisms leading to paranoia, contributing to the understanding of psychotic disorders and the impact of cannabis use on mental health.
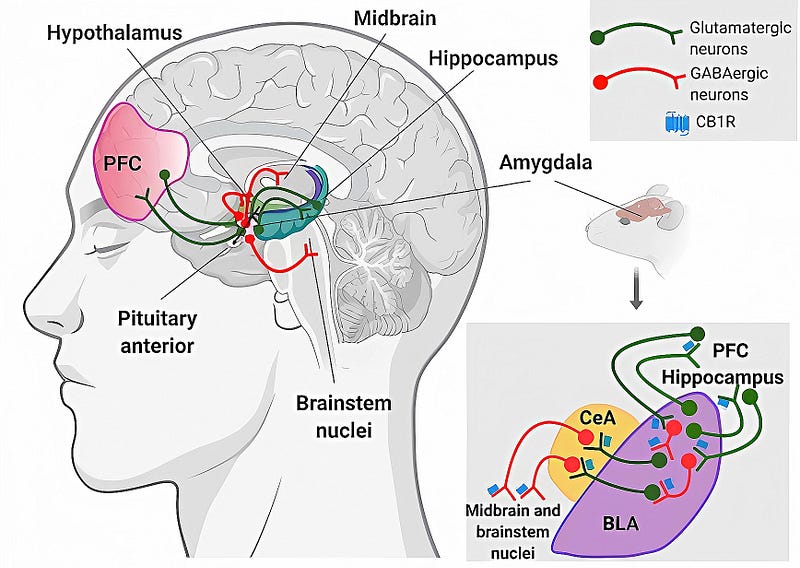
Concurrently, THC disrupts glutamatergic neurotransmission and GABAergic inhibitory circuits, leading to a state of cortical disinhibition and aberrant salience attribution. In this state, neutral stimuli may be misinterpreted as personally significant or threatening, forming the neurochemical basis for paranoid ideation. Furthermore, individuals with a genetic predisposition to psychosis, often involving genes related to dopamine metabolism such as COMT, may exhibit heightened sensitivity to these THC-induced neurochemical disruptions. The role of cannabidiol (CBD), another major phytocannabinoid, is particularly noteworthy for its potential protective effects. CBD is thought to act as a negative allosteric modulator of the CB1 receptor and may mitigate the anxiogenic and psychotogenic impacts of THC, suggesting that the THC-to-CBD ratio in consumed products is a critical determinant of risk.
Epidemiology and Risk Factors
The prevalence of cannabis-induced paranoia varies significantly across studies, influenced by methodology, population studied, and cannabis use patterns. Large-scale surveys indicate that approximately twenty to thirty percent of recreational users report experiencing paranoid thoughts during intoxication. Specific risk factors have been consistently identified that modulate individual vulnerability. Adolescent onset of use is a major risk factor, as the adolescent brain, particularly the prefrontal cortex, is undergoing critical development and is highly susceptible to the disruptive effects of THC on neurodevelopmental processes.
The potency of cannabis products is perhaps the most significant modifiable risk factor. The widespread availability of high-potency concentrates and sinsemilla flower, with THC concentrations often exceeding twenty percent, has been directly linked to increased rates of psychiatric emergency department presentations for psychosis and paranoia. Dose-dependent relationships are clearly established, with higher cumulative THC exposure correlating linearly with increased risk for psychotic symptoms.
User-specific factors are equally critical. Individuals with a personal or family history of psychosis, anxiety disorders, or mood disorders are at substantially elevated risk. A history of childhood trauma or adversity also significantly increases vulnerability, potentially through lasting effects on the hypothalamic-pituitary-adrenal (HPA) axis and stress response systems. The context of use is also important; using cannabis to self-medicate negative mood states is a strong predictor of adverse psychological effects, including paranoia, likely due to pre-existing psychological vulnerabilities.
Clinical Presentation and Assessment
The clinical presentation of cannabis-induced paranoia typically occurs during acute intoxication or shortly thereafter. Symptoms range from mild ideas of reference, such as believing people are talking about them, to severe, fixed persecutory delusions that can necessitate emergency intervention. These symptoms are often accompanied by other features of intoxication, including anxiety, panic, depersonalization, derealization, and cognitive impairments in memory, attention, and executive function.
A thorough clinical assessment is paramount. This must include a detailed history of substance use, specifying the type of product (e.g., flower, concentrate, edible), estimated potency, frequency, and pattern of use. The temporal relationship between cannabis use and symptom onset must be established to differentiate substance-induced symptoms from a primary psychiatric disorder. Collateral history from family or friends is often invaluable. Standardized diagnostic interviews and rating scales for psychotic symptoms can aid in objective assessment. A crucial diagnostic challenge lies in the overlap between cannabis-induced psychosis and the prodromal or acute phases of a primary psychotic disorder, a distinction that often requires observation over time and abstinence from cannabis.
Conclusion and Public Health Implications
Cannabis-induced paranoia is a common and clinically significant adverse effect of THC that arises from a complex interaction between a powerful psychoactive compound and individual neurobiological and psychological vulnerabilities. The neuropathology involves a cascade of dysregulation across dopaminergic, glutamatergic, and endocannabinoid systems. The modern landscape of high-potency cannabis products poses a greater public health threat than the lower-potency products studied in previous decades.
There is an urgent need for targeted public health initiatives. These must include evidence-based education on the psychiatric risks of high-potency cannabis, particularly aimed at adolescents and individuals with pre-existing mental health conditions. Regulatory policies should consider mandating limits on THC potency and requiring clear labeling of cannabinoid content, including THC and CBD percentages, to inform consumer choice. For clinicians, heightened vigilance, routine screening for cannabis use in psychiatric settings, and the implementation of harm-reduction strategies are essential. Future research must prioritize longitudinal studies to clarify the long-term outcomes of cannabis-induced paranoia and its relationship to chronic psychiatric conditions, as well as explore potential pharmacological and psychotherapeutic interventions for affected individuals.