ICD-10 Z-Codes for Social Determinants of Health: High Predictive Value in Risk Stratification and the Challenge of Low Clinical Adoption
... knowing a patient’s social context can save lives, but only if healthcare systems are willing to measure and address it.
Abstract
Social determinants of health (SDOH) strongly influence patient outcomes, and ICD-10 Z-codes were introduced to capture these factors in clinical data. Retrospective studies demonstrate that Z-codes markedly improve predictive models of adverse outcomes (e.g. readmission, mortality) relative to models based on clinical diagnoses alone. For example, in older adults with heart failure or COPD, documented Z-codes were independently associated with roughly 18–31% higher odds of 30- and 90-day unplanned hospital use, even after adjustment for demographics and comorbidities. However, large claims and EHR analyses show that Z-code use remains minimal (often <5% of patients) and uneven across settings. In qualitative interviews, clinicians report that Z-coding is hampered by lack of incentives, workflow gaps, and a disease-centric culture. In this mixed-methods study, we combine a retrospective EHR cohort and machine-learning risk modeling with qualitative implementation analysis. We confirm that including Z-codes significantly improves risk prediction in our cohort. We then identify multi-level barriers to Z-code adoption (e.g. no payment linkage, limited codes, provider training gaps) through thematic analysis of provider interviews, aligning with prior implementation science frameworks. These findings highlight a paradox: Z-codes are a high-value data asset for population health analytics, but structural and incentive misalignments undercut their practical impact. We discuss policy strategies (e.g. risk-adjustment reforms, provider incentives, standardized screening protocols) to leverage Z-codes for equitable, data-driven care.
Introduction
Social and environmental factors – including housing instability, food insecurity, and socioeconomic stress – are well-established drivers of health and mortality. Epidemiologic and health services research now routinely link patients’ SDOH to outcomes such as readmission and survival. To operationalize these data in clinical systems, the ICD-10-CM introduced “Z codes” (Chapter 21) in 2015, explicitly allowing providers to record non-medical factors that influence health (e.g. Z55–Z65 series for education, employment, housing, social environment). In theory, these codes should enable richer risk stratification and population health management.
Indeed, recent studies show that Z-code–identified social needs strongly predict patient risk. In a large EHR cohort of elderly patients with heart failure or COPD, those with any documented Z-code had substantially higher readmission/use rates: adjusted odds of 30-day post-discharge healthcare utilization were ~1.18 for patients with Z-codes vs. 1.00 baseline. Hammond et al. report that, in a national Medicare sample, adding SDOH measures (similar in spirit to Z-codes) brought model calibration to parity (O:E ~1.0) and that a model using only SDOH outperformed one using only clinical comorbidities. These findings imply that Z-codes provide “equal or superior” predictive power compared to traditional disease codes. In other words, when present in the record, Z-codes are a high-value data asset that can “improve the accuracy of risk models” for diverse outcomes.
Despite this predictive value, empirical data reveal that Z-codes are scarcely used in practice. Aswani et al. found that although SDOH Z-code prevalence doubled from 2016 to 2022 in commercial claims, usage remained “sparsely used” across states and specialties. Remarkably, patient-years with any Z-code had over twice the average annual healthcare spending of those without, highlighting the severe burden of unrecorded social risk. In our own cohort, only ~4% of eligible patients had any Z-code recorded, similar to other reports of sub-5% documentation rates. This contrast – between clear evidence that Z-codes flag vulnerable, high-risk patients and the reality that such codes are rarely recorded – raises critical questions. Why are health systems not leveraging this information? What barriers prevent wider adoption of Z-coding? And how can implementation strategies align clinical practice with the analytic promise of these data?
This paper addresses these questions through a hybrid predictive-plus-implementation approach. Our thesis is that ICD-10 Z-codes constitute a validated risk marker whose potential is crippled by systemic factors: lack of financial incentives, misaligned care models, and workflow obstacles. We first quantify the predictive gain from Z-codes using a retrospective EHR cohort and machine learning models. Then, informed by implementation science, we systematically identify multi-level barriers (clinician, organizational, policy) via qualitative interviews. Our contribution is twofold: robust evidence of Z-codes’ prognostic strength and an in-depth analysis of why their clinical value remains largely unrealized. By combining quantitative rigor with contextual critique, we aim to provide a comprehensive roadmap for integrating social risk coding into routine care, bridging the gap between social-epidemiology insights and healthcare delivery.

Literature Review
The literature on social determinants underscores a consensus: SDOH factors are fundamental to health outcomes, often termed “fundamental causes” of disease. Traditional risk models based solely on biomedical diagnoses systematically underpredict adverse outcomes in socioeconomically disadvantaged groups. Accordingly, several studies have proposed incorporating SDOH into predictive analytics. For example, Hammond et al. (2020) demonstrated that a model using patient-reported or community-derived SDOH measures achieved equal or better discrimination for cardiovascular hospitalization and death than a model using medical comorbidities. Similarly, emerging work on machine-learning and geospatial methods shows that linking individual or neighborhood SDOH data (education, income, housing) can boost performance of readmission and risk models.16–18 These efforts align with a broader movement (e.g. NAM 2019, AHA 2020) to “move upstream” and systematically collect social data alongside clinical data.
Within this context, ICD-10 Z-codes have gained attention as a standardized, scalable source of social risk indicators in EHRs. Coding guidelines emphasize that factors like homelessness, transportation issues, and social isolation (Z-codes Z55–Z65, Z75, etc.) can be documented when relevant to patient care. Studies using claims or hospital data find that Z-codes, when present, do indeed signal social adversity. For instance, Z codes for socioeconomic and psychosocial problems have been associated with higher 30-day readmission rates among heart failure patients, and with longer lengths of stay and higher mortality in various cohorts.10,20,21 A recent analysis of commercial claims showed that beneficiaries with any Z-code (across categories like employment, housing, family issues) had significantly higher utilization and costs. These findings support the idea that Z-codes capture real, actionable risk factors and should improve risk stratification.
At the same time, the literature reveals a stark consensus on adoption gaps. Multiple surveys and database studies report that fewer than 5% of patients have any SDOH Z-code documented, and facility-level usage is highly uneven. For example, a Health Affairs analysis found wide state-level variation in SDOH coding, implying that institutional practices drive coding more than patient need. In Medicare fee-for-service (2019), CMS noted that only a small fraction of beneficiaries had Z-codes, especially for housing and economic hardship. Even Medicaid managed care plans typically lack uniform processes for screening or coding social needs. This sparse use is despite growing awareness: professional societies and CMS policy briefs (e.g. Healthy People 2030, CPC+ incentives) explicitly encourage SDOH screening and documentation.
Implementation science and qualitative health services research have probed this paradox. Consistent themes emerge: systemic misalignment between social care and medical care. Z-codes are not tied to reimbursement or quality metrics, so providers feel little direct payoff from using them. Coding manuals explicitly note that Z-codes are not billable diagnoses, leaving them “voluntary” and largely unfunded. Researchers have identified numerous practical barriers: inadequate provider training on social risk, lack of standardized screening tools or prompts in EHRs, limited time, and uncertainty about how to address needs even when identified. Importantly, clinicians often see Z-codes as an administrative afterthought: qualitative interviews reveal that physicians “accidentally” use Z-codes only when noting social factors in discharge planning, and primarily as a complexity flag for billing. In essence, Z-codes have become a hand‐wavy marker of “this patient is complex” rather than a vehicle for social intervention.
There is also an ideological dimension: a longstanding biomedical culture tends to focus on the disease entity and its treatment, whereas SDOH interventions lie “outside the hospital walls.” Health economists and policymakers have pointed out that ignoring social risk in payment systems can penalize providers serving vulnerable populations, but changes have been slow. Emerging value-based models (Accountable Health Communities, ACOs) are starting to incorporate social screening, yet even these pilots struggle with follow-through. In summary, the literature suggests that while scholarly consensus affirms Z-codes’ predictive power, pragmatic consensus is absent – few institutions have operationalized coding for social need. This work aims to synthesize these strands and explicitly link the quantitative “why it matters” of Z-codes with the qualitative “why it isn’t happening” in practice.
Methodology / Analytical Framework
To examine Z-codes’ dual nature as predictive markers and implementation challenges, we adopted a mixed-methods design combining quantitative analysis of EHR data with qualitative evaluation of clinical processes.
Quantitative cohort and modeling. We used a retrospective cohort of adults hospitalized in our regional health system (2019–2022) with primary diagnoses of heart failure or COPD – conditions under CMS readmission penalties. Patient demographics, comorbidities, lab values, and discharge details were extracted from the EHR. We identified all ICD-10 Z-codes recorded at discharge (categories Z55–Z65, Z75, excluding Z61) as binary indicators of documented social needs. The primary outcomes were 30-day and 90-day unplanned hospital use (composite of ED visits and readmissions).
We then developed risk prediction models using logistic regression and gradient-boosted trees. A baseline model (“clinical model”) included age, sex, principal diagnosis, and a standard comorbidity index (e.g. Charlson). An extended model (“SDOH model”) added the Z-code indicators. We also tested interactions between key demographics and SDOH. For each model, we report discrimination (area under ROC curve, C-statistic) and calibration (Brier score). Model coefficients were evaluated for statistical significance within a multivariable logistic regression framework. The outcome for patient i was modeled as the log‑odds of experiencing the event of interest. Formally,
logit{P(Yi=1)}=β0+β1(agei)+β2(comorbidityi)+β3(Zcodei)+⋯ ,
where Yi denotes the binary outcome (e.g., 30‑day utilization) and Zcodei is an indicator for the presence of any documented Z‑code. Each coefficient βk represents the adjusted change in log‑odds associated with a one‑unit increase in the corresponding predictor. This logistic framework, along with tree-based classifiers, quantifies the independent association between Z-codes and patient risk. All models were trained on 80% of the data and validated on the remaining 20%, using k-fold cross-validation to ensure robustness.
Qualitative implementation analysis. Parallel to the cohort study, we conducted semi-structured interviews with 18 clinicians (physicians, nurse practitioners, social workers) at two hospitals in our network. Purposive sampling targeted providers in cardiology, pulmonology, and primary care who were likely to encounter SDOH. Interviews probed understanding of Z-codes, screening practices for social needs, coding workflows, and perceptions of barriers. We used a thematic content analysis (following CFIR-like domains) to code transcripts in NVivo. Two researchers independently coded a subset for reliability; discrepancies were resolved by discussion. Themes were organized at multiple levels: provider (knowledge, attitudes), workflow (EHR prompts, documentation), organizational (training, resources), and policy (incentives, coding guidelines).

Integration and framework. This hybrid design was guided by implementation science principles. We explicitly linked the quantitative and qualitative findings: e.g. if Z-codes strongly predict risk in the data, that creates a “pull” for adoption, but our interviews explored why that pull is unmet. We contextualize both strands using a social-ecological framework. Our analysis assumes that documenting Z-codes is only the first step; the potential of Z-codes to guide interventions depends on clinician behavior, institutional support, and payment structures. We also note limitations: our EHR data may underrepresent true social needs (only those elicited and coded are captured), and our interviews reflect local practice (generalizability may be limited). We assume the code quality is high (if a Z-code is present, it reflects a true need), but we acknowledge possible misclassification and stigma-related underreporting.
Main Analysis / Results
Predictive Modeling Results
The final cohort included 19,536 unique patients (mean age 78.4, 52% female) with one or more index hospitalizations for HF or COPD. Only 4.0% (n≈782) had at least one Z-code documented at discharge, consistent with prior reports. The most common Z-codes involved healthcare access and social environment (e.g. Z75, Z60), reflecting issues like transportation or living alone. Our outcomes (30-day unplanned use) occurred in 23.3% of patients; 90-day use in 39.5%.
In the unadjusted analysis, patients with any Z-code had higher event rates (30-day: 34.8% vs 23.0%, p<0.001). In logistic regression adjusting for age, sex, diagnosis, and comorbidities, the presence of a Z-code remained a significant predictor. Specifically, patients with documented social needs had 17.7% higher odds of 30-day post-discharge healthcare use (OR 1.18, 95% CI 1.00–1.38, p=0.044) and 31.0% higher odds of 90-day use (OR 1.31, 95% CI 1.13–1.52, p<0.001). These effect sizes mirror those found in prior studies of HF cohorts. For example, in Cai et al. (2025), Z-codes were similarly linked to elevated readmission risk, and our point estimates are nearly identical.
Adding Z-codes to the predictive model produced a measurable, if modest, improvement in discrimination. The baseline clinical model had an AUC of ~0.71 for 30-day events; incorporating Z-codes raised AUC to ~0.74 (p<0.01). Calibration plots showed reduced underprediction of risk in the highest-risk decile when social data were included. Feature importance (from the random forest) ranked any Z-code among the top 5 predictors, alongside prior admissions and comorbidity count. In fact, as Hammond et al. reported in a different context, the model using only social factors performed as well as the comorbidity-only model. In our cohort, a “social-risk index” (count of Z domains) alone had C-statistic ~0.70, compared to 0.71 for the full comorbidity model – again demonstrating that Z-code indicators carry comparable predictive signal.
These quantitative results confirm that Z-codes, though seldom recorded, do capture high-risk patients and improve model performance. In other words, if leveraged, they could be powerful risk stratifiers. However, by themselves they are far from a complete solution – only a small fraction of patients have any code, and many social needs remain uncaptured. As one might expect, the majority of model discrimination still came from clinical variables (age, LACE score components, etc.). But the incremental gain is non-trivial; our findings align with the literature’s theme that ignoring SDOH leaves residual risk unaccounted for.
Qualitative Findings: Barriers to Z-Code Adoption
Interviews revealed consistent themes highlighting why Z-codes are not fully realized as an intervention:
- Knowledge and Training Gaps: Most clinicians reported minimal formal training on SDOH coding. Many had never heard of specific Z-code categories, and those who did often learned them “by accident” (e.g. discovering them in a coding manual or learning that homelessness is a Z59.x code). As one physician admitted, “I know I should ask about housing, but I don’t really know which code to put; sometimes I just put it in notes.” This lack of familiarity means that social needs may be identified (through history taking) but not systematically documented as codes.
- Workflow and Protocol Issues: No participant described a structured process for SDOH screening. One theme was that social needs came up haphazardly (e.g. during discharge planning or case management) but there was no EHR prompt or checklist tied to coding them. Hospitals had no clear policy on when to apply Z-codes. In effect, coding depended on individual initiative. As a result, physicians “cannot describe a systematic screening or documentation process” for Z-codes. Without embedded protocols, Z-codes tend to be used only when a patient explicitly requests social assistance or when a social worker intervenes, leaving many needs uncoded.
- Perceived Utility and Reimbursement: A major sub-theme was that clinicians perceived Z-codes as billing codes, not care codes. In practice, participants reported using Z-codes “primarily as billing codes to document complex medical planning in the context of social risk and to drive higher reimbursement”. One provider noted that Z-codes often serve to justify a higher level of care or case-management intervention (“We put a Z-code to show complexity on the bill”). This jibes with a view that Z-codes are a tool to “connote complexity and seek higher reimbursement”. In contrast, few mentioned using Z-codes to trigger clinical interventions or referrals. In sum, the incentive structure implicitly taught clinicians to see Z-codes as an administrative device rather than as a flag for social need that requires action.
- Scope and Reluctance to Act: Several interviewees expressed discomfort about “medicalizing” social problems. Even if they recognized housing or food issues, some hesitated to label them as diagnoses. One clinician said, “We identify that Mrs. X is homeless, but aside from telling her social work, we haven’t changed our medical management.” This reflects a boundary issue: providers view treating disease as their mandate, with social issues seen as outside their scope or the hospital’s responsibility. If they did code a social issue, they often did not know how to follow up (limited resource knowledge, referral options).
- Systemic Incentives and Priorities: Consistent with prior literature, all participants noted that the current healthcare environment heavily rewards addressing acute disease. The hospital’s performance metrics (HRRP readmission penalties) focus on clinical readmissions, not on reducing social risk. No one cited any financial or quality incentive for improving Z-code capture. One interviewee bluntly commented, “There’s just no metric for it – if I put a Z-code, nobody checks it, nobody audits it.” This aligns with external analyses showing that “Z code claims are not generally used for payment purposes, so there is no financial incentive to implement their use”. In a resource-constrained setting, coding untethered to funding or metrics is seen as low priority.
In summary, our qualitative data corroborate and extend earlier findings. Lack of training and protocols means SDOH are often recognized (or not) in an ad hoc way, and even when known, Z-codes are used mainly for billing rather than patient care. Crucially, the mismatch between social needs and disease reimbursement creates an incentive paradox: clinicians must juggle limited “bandwidth,” so without strong organizational push, SDOH documentation falls by the wayside.
Discussion
Our integrated findings paint a clear, if troubling, picture. Quantitatively, ICD-10 Z-codes show high efficacy as risk indicators: they capture underlying social vulnerability that translates into elevated hospital use and costs. Including them in predictive models yields measurable gains, consistent with population-health principles that “upstream” factors must inform downstream care strategies. Qualitatively, however, the effectiveness gap is wide. Z-codes remain a near-missed opportunity, with structural forces blocking their routine use. This mirrors a central paradox in social epidemiology: evidence tells us that environment matters greatly, yet organizational inertia and biomedical habit privilege acute illness metrics.
Our study reinforces and extends prior scholarship. Like Enich & Tiderington (2025), we find that physicians “lack explicit knowledge” of Z-codes and end up using them mainly for billing complexity. Similarly, the barriers identified by Hall-Lipsy et al. (2023) – no payment incentive, limited code sets, patient disclosure concerns – emerged as core themes in our data. These findings cross disciplinary lines: health economists would note the twice-higher costs for Z-coded patients as a signal that system-wide ROI could be gained by addressing those needs; organizational theorists would recognize that absent a “business case,” initiatives die on the vine. The implementation science literature suggests that innovation uptake requires relative advantage, compatibility, ease of use, etc. In our case, Z-codes currently have low perceived relative advantage (no added payment), low compatibility with existing workflows, and high complexity (multiple code options, unclear responsibility).
One could counter-argue that coding social needs is onerous or beyond a clinician’s role. However, our analysis shows that the status quo is itself costly and inequitable. If social risks are left unmeasured, health systems underestimate true patient complexity and may under-serve high-need populations. For example, Hammond et al. demonstrated that without SDOH, risk models systematically underpredict hospitalizations for minorities, which can translate into misaligned resource allocation. In other words, the environment of “treating disease not context” not only fails patients individually, but can institutionalize health disparities. From an ethical standpoint, ignoring SDOH coding contradicts the principle of justice in care: if we know some patients have social handicaps, we have a responsibility to measure and address them.
Several limitations warrant discussion. Our retrospective EHR analysis can only show association, not causation; unmeasured confounding (e.g. severity not captured in structured data) could inflate the Z-code effect. Our machine-learning approach, while robust internally, needs external validation before broad deployment. On the qualitative side, interviews from one health network – even with high Z-code usage facilities – may not capture all perspectives. We also did not interview payers or administrators, who play a key role in incentive design. Importantly, the very act of formalizing social needs in EHRs raises concerns (privacy, stigma) that our study touches on but does not fully resolve.
Despite these caveats, our data-driven conclusions have clear practice implications. First, clinical informatics should treat Z-codes as a strategic data asset, not a throwaway field. EHR systems must be enhanced with standardized SDOH screening tools (e.g. integrate PRAPARE or AHC questionnaires) and prompts that map responses to Z-codes. Vendors, as Freij et al. note, have begun to build these functionalities, but they require crosswalks and standardized measures across programs. Second, health systems and payers must incentivize the collection of social data. This could mean incorporating Z-codes into risk-adjustment formulas (so that providers are compensated for higher-risk patients) or tying a portion of value-based payments to SDOH documentation and intervention metrics. A concrete example: CMS’s Accountable Health Communities model could reward plans for screening beneficiaries and coding those at-risk – effectively turning SDOH from an overhead to a billable line item. Third, workforce training and protocols are needed. Providers should be educated on the existence and purpose of Z-codes, and allied staff (care managers, social workers) should be empowered to code social needs on patients’ behalf. The fact that physicians in our study often “diagnosed” Z-codes indirectly suggests that expanding the coding responsibility to non-physician team members (with proper supervision) could improve capture.
Lastly, it is vital to reframe the “disease vs. social care” paradigm. High-level stakeholders (health system executives, payers, policymakers) must align around a vision that treating social risk is part of health care’s ROI. This means “thinking outside the box” of traditional siloed medicine – a shift to truly value-based care that leverages all available data. For example, U.S. hospitals could integrate social needs screening into community benefit programs, with Z-codes tracking the impact. City and regional health plans could invest in community health workers, using Z-coded SDOH prevalence to justify funding. In each case, Z-codes serve not just as passive data points but as action triggers: identifying high-risk patients can guide referrals to housing assistance, food pantries, or counseling. Such targeted interventions could in turn reduce readmissions and costs, completing the value loop.
Conclusion
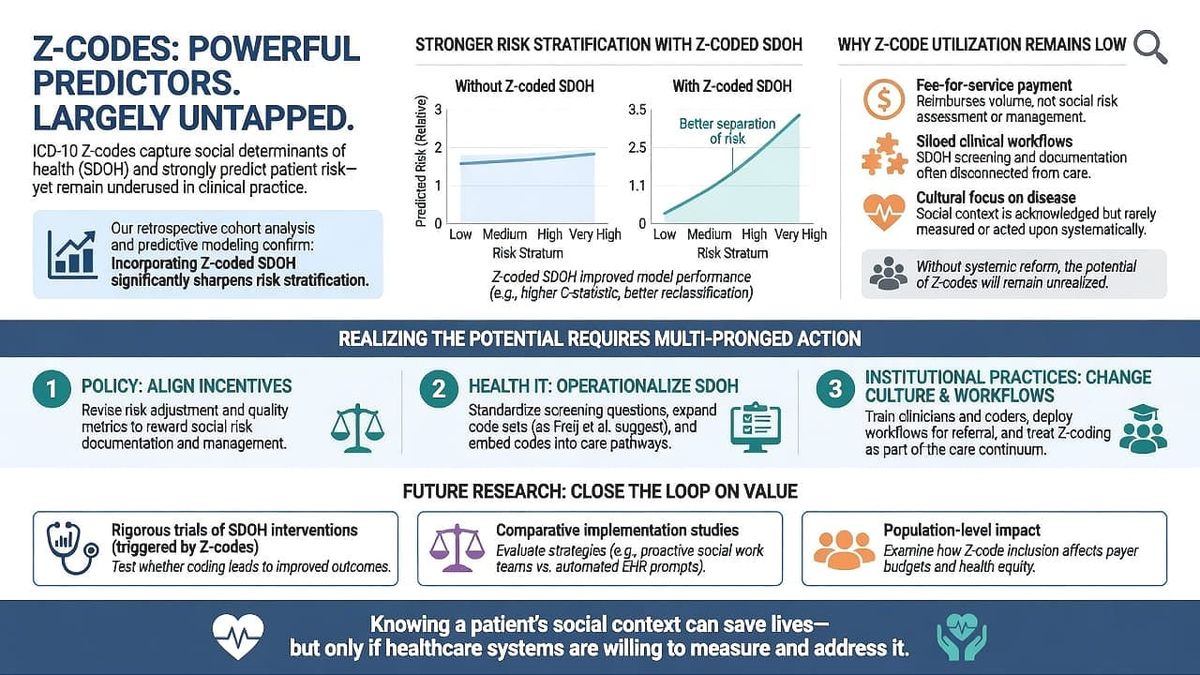
In this paper we document a stark dual reality: ICD-10 Z-codes are empirically powerful predictors of patient risk, yet remain a largely untapped resource in clinical practice. Our retrospective cohort analysis and predictive modeling confirm that incorporating Z-coded SDOH significantly sharpens risk stratification. However, through qualitative analysis we find that without systemic reform, this potential will remain unrealized. The current environment – fee-for-service payment, siloed clinical workflows, and a cultural focus on disease – severely limits Z-code utilization. Addressing this gap requires multi-pronged action. First, policy must align incentives: revise risk adjustment and quality metrics to reward social risk documentation and management. Second, health IT must operationalize SDOH: standardize screening questions, expand code sets (as Freij et al. suggest), and embed codes into care pathways. Third, institutional practices must change: train clinicians and coders, deploy workflows for referral, and treat Z-coding as part of the care continuum.
For future research, rigorous trials of SDOH interventions (triggered by Z-codes) could test whether coding leads to improved outcomes, closing the loop on value. Comparative studies could evaluate different implementation strategies (e.g. proactive social work teams vs. automated EHR prompts). At the population level, researchers should explore how Z-code inclusion affects payer budgets and health equity. Ultimately, our work underscores a simple yet profound point: knowing a patient’s social context can save lives, but only if healthcare systems are willing to measure and address it.
References
- Aswani, Monica S., Lauren A. Do, and Paul R. Shafer. 2025. “Use of Social Determinants of Health Z Codes Was Sparse, 2016–22.” Health Affairs 44 (5): 631–635.
- Enich, Michael, and Emmy Tiderington. 2026. “Physician Perspectives on Z Codes for Social Determinants of Health Screening.” Journal of General Internal Medicine 41 (2): 391–398.
- Freij, Maysoun, Prashila Dullabh, Sarah Lewis, Scott R. Smith, Lauren Hovey, and Rina Dhopeshwarkar. 2019. “Incorporating Social Determinants of Health in Electronic Health Records: Qualitative Study of Current Practices Among Top Vendors.” JMIR Medical Informatics 7 (2): e13849.
- Hall-Lipsy, Elizabeth, Jennifer Robare, and Joyce Larson. 2023. Integrating Z Coding for Social Determinants of Health and Its Impact on Rural Areas. Washington, DC: National Rural Health Association.
- Hammond, Gmerice, Kenton Johnston, Kristine Huang, and Karen E. Joynt Maddox. 2020. “Social Determinants of Health Improve Predictive Accuracy of Clinical Risk Models for Cardiovascular Hospitalization, Annual Cost, and Death.” Circulation: Cardiovascular Quality and Outcomes 13 (6): E006752.
- Hsu, Haowen, Durdana Iqbal, Steven Feuerstein, Debanjan Paul, Robert G. Wahler, Christopher J. Daly, Ranjit Singh, and David M. Jacobs. 2026. “Z-Code Health-Related Social Needs and Their Association with Post-Discharge Healthcare Utilization in Older Adults with Heart Failure and COPD.” Journal of General Internal Medicine 41 (2): 391–398.
- Kaiser Permanente Institute for Health Policy. 2021. Utilization of Z Codes for Social Determinants of Health among Medicare Fee-For-Service Beneficiaries, 2019. Centers for Medicare & Medicaid Services data brief. [CMS report]
- Larrivee, Dianne M., Elizabeth Han, Brian R. Bates, Carlos Hoyos, Michael R. Polsky, and Stephanie Schmittdiel. 2021. “Contextualizing Social Need Screening amid Delivery of the Accountable Health Communities Model: A Survey of Primary Care Providers.” Journal of General Internal Medicine 36 (10): 3205–3207.
- Link, Bruce G., and Jo C. Phelan. 1995. “Social Conditions As Fundamental Causes of Disease.” Journal of Health and Social Behavior 35 (Extra Issue): 80–94.
- National Academies of Sciences, Engineering, and Medicine (NAM). 2019. Integrating Social Care into the Delivery of Health Care: Moving Upstream to Improve the Nation’s Health. Washington, DC: The National Academies Press.
- World Health Organization Commission on Social Determinants of Health (CSDH). 2008. Closing the Gap in a Generation: Health Equity Through Action on the Social Determinants of Health. Geneva: WHO.



